Cut, Close, or Consult?
A Case-Based Approach to Skin Cancer for Plastic Surgeons
2026-05-27
Let’s Calibrate the Room
Raise your hand if you are a
graduating senior
This may change how much dermatology trivia I inflict on you.
Let’s Calibrate the Room
Raise your hand if you are a
medical student
.
Let’s Calibrate the Room
Raise your hand if you have
diagnosed and/or treated melanoma
.
Let’s Calibrate the Room
Raise your hand if you have
diagnosed and/or treated CSCC
.
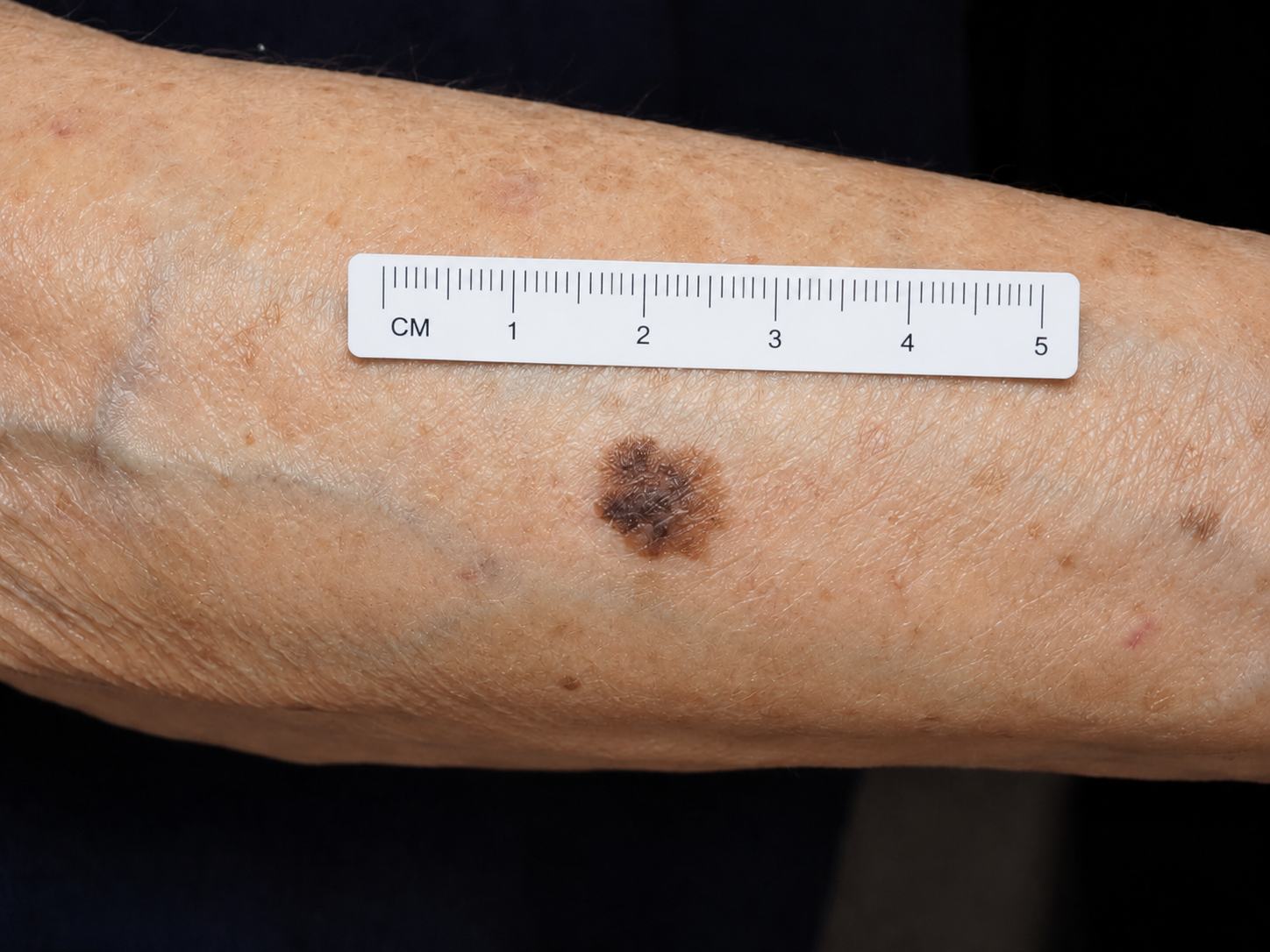
Case 1: Pigmented Lesion on the Forearm
A 72-year-old woman presents with a pigmented lesion on the right forearm.
She is unsure how long it has been present, but thinks it may have changed over time.
Cut or Consult?
What should happen next?
- Shave biopsy
- Punch biopsy
- Excisional biopsy
- Wide local excision
- Refer before biopsy
Answer: Excisional Biopsy
Why? Because the biopsy is the first staging procedure.
For a lesion suspicious for melanoma, the goal is to obtain:
- The entire lesion
- Full-thickness sampling
- Accurate Breslow depth
- Peripheral and deep margin status
Practical answer: narrow excisional biopsy with ~1–3 mm margins.
Case 2: Slowly Growing Pigmented Patch on the Cheek
A 75-year-old woman presents with a slowly growing, asymptomatic pigmented patch on the right cheek.
She is unsure when it first appeared, but believes it has gradually enlarged over several years.

Cut or Consult?
What is the best next step?
- Broad shave biopsy
- Excisional biopsy
- Multiple scouting biopsies
- Refer to dermatology for dermoscopy / confocal microscopy
Practical Answer: Consult, Then Targeted Scouting Biopsies
Large pigmented facial patch
suspicious for lentigo maligna / LMM
This is not the lesion to broadly shave in its entirety.
For a 4–5 cm facial lesion, the practical next step is:
Consult
Dermoscopy ± confocal → targeted scouting biopsies of the most atypical areas
Practical Answer: Consult, Then Targeted Scouting Biopsies
Large pigmented facial patch
suspicious for lentigo maligna / LMM
Why?
- The lesion is large
- The site is cosmetically sensitive
- Complete excisional biopsy is impractical
- A broad shave of the entire lesion would be unnecessarily destructive
Biopsy goal: confirm LM/LMM and rule out focal invasion before definitive margin-controlled surgery.
Case 1 Continued: The Pathology Returns
The forearm lesion was sampled with a narrow excisional biopsy.
The patient returns to discuss the pathology.
Pathology Report
Diagnosis: Superficial spreading melanoma
Breslow thickness: 1.6 mm
Ulceration: Not identified
Mitotic rate: 1/mm²
Microsatellites: Not present
Tumor-infiltrating lymphocytes: Present, non-brisk
Margins: Inked margins negative
Pathologic T category: pT2a
Let’s Calibrate the Room
Raise your hand if you have
used a melanoma risk stratifying algorithm
.
Risk Stratification: Stage II Melanoma
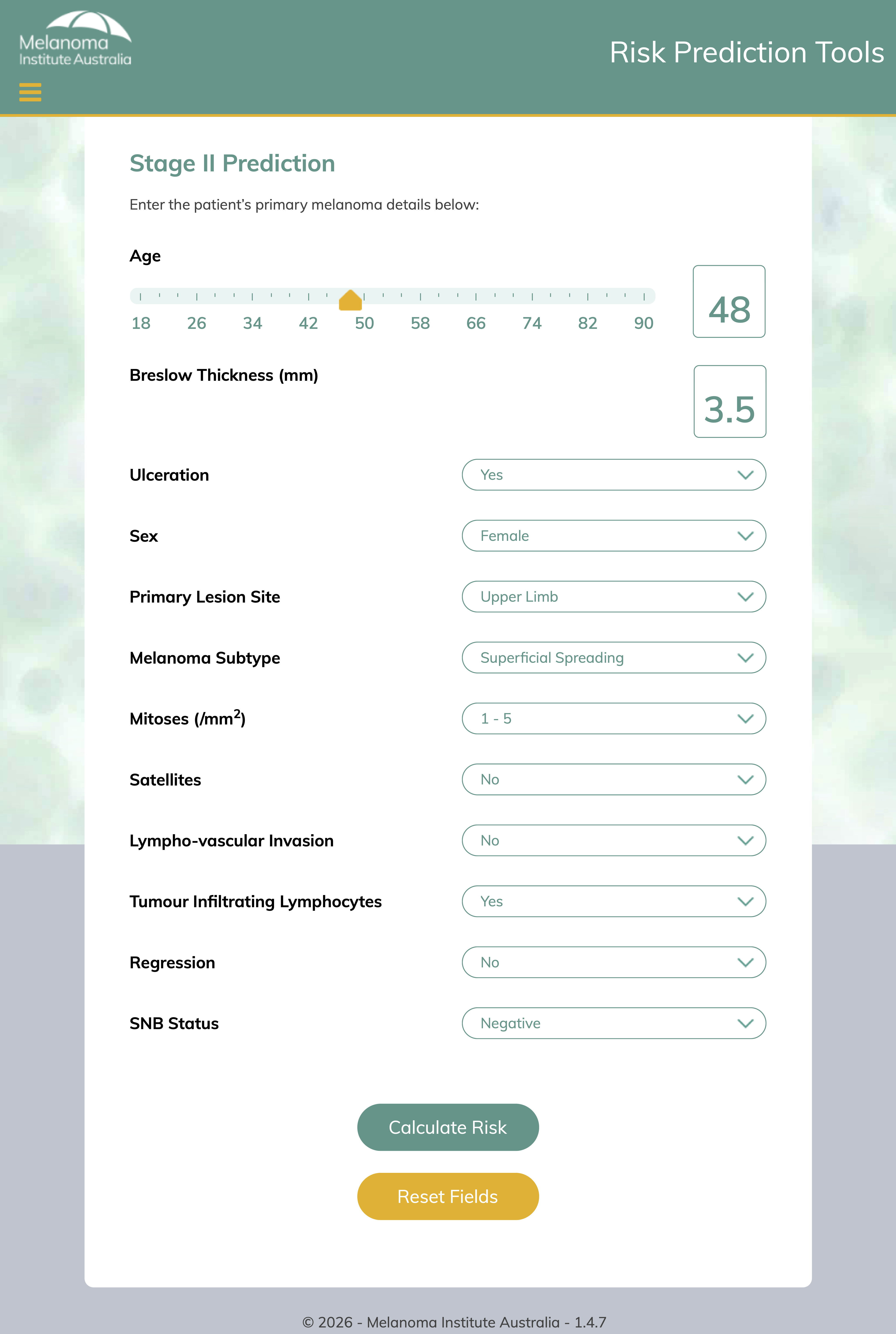
Risk Stratification Changes the Conversation
This is node-negative melanoma.
Estimated risk is still meaningful.
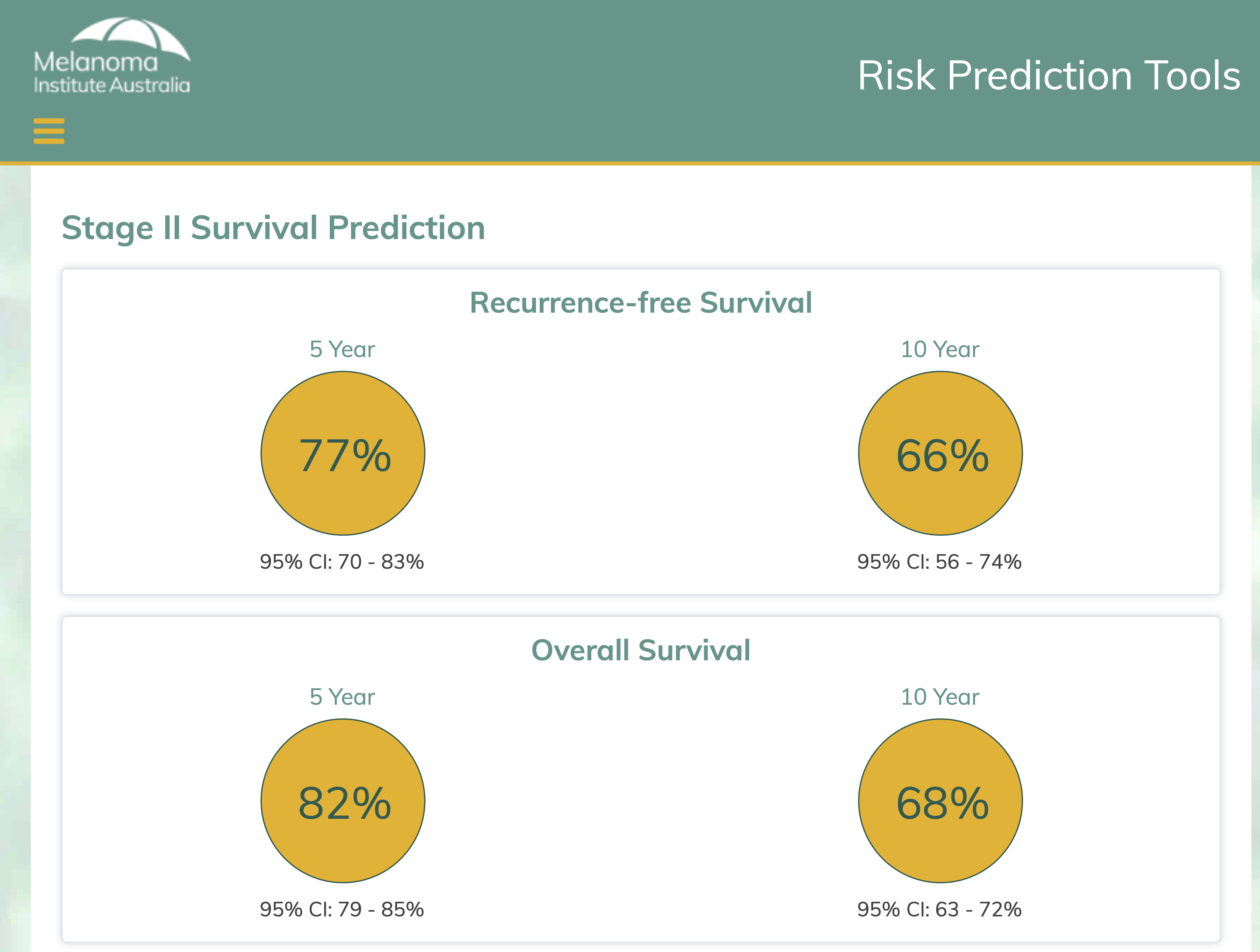
Estimated 10-year RFS: 66%
That means recurrence risk is roughly 1 in 3 over 10 years.
Case 4: Forehead CSCC
An 82-year-old woman with numerous prior NMSCs presents with a new lesion on the left forehead.
Physical exam:
- 1.3 cm
- No clinical adenopathy
Biopsy shows:
- Well-differentiated CSCC

Question: cut & close, or consult?
How Do We Assess the Margin?
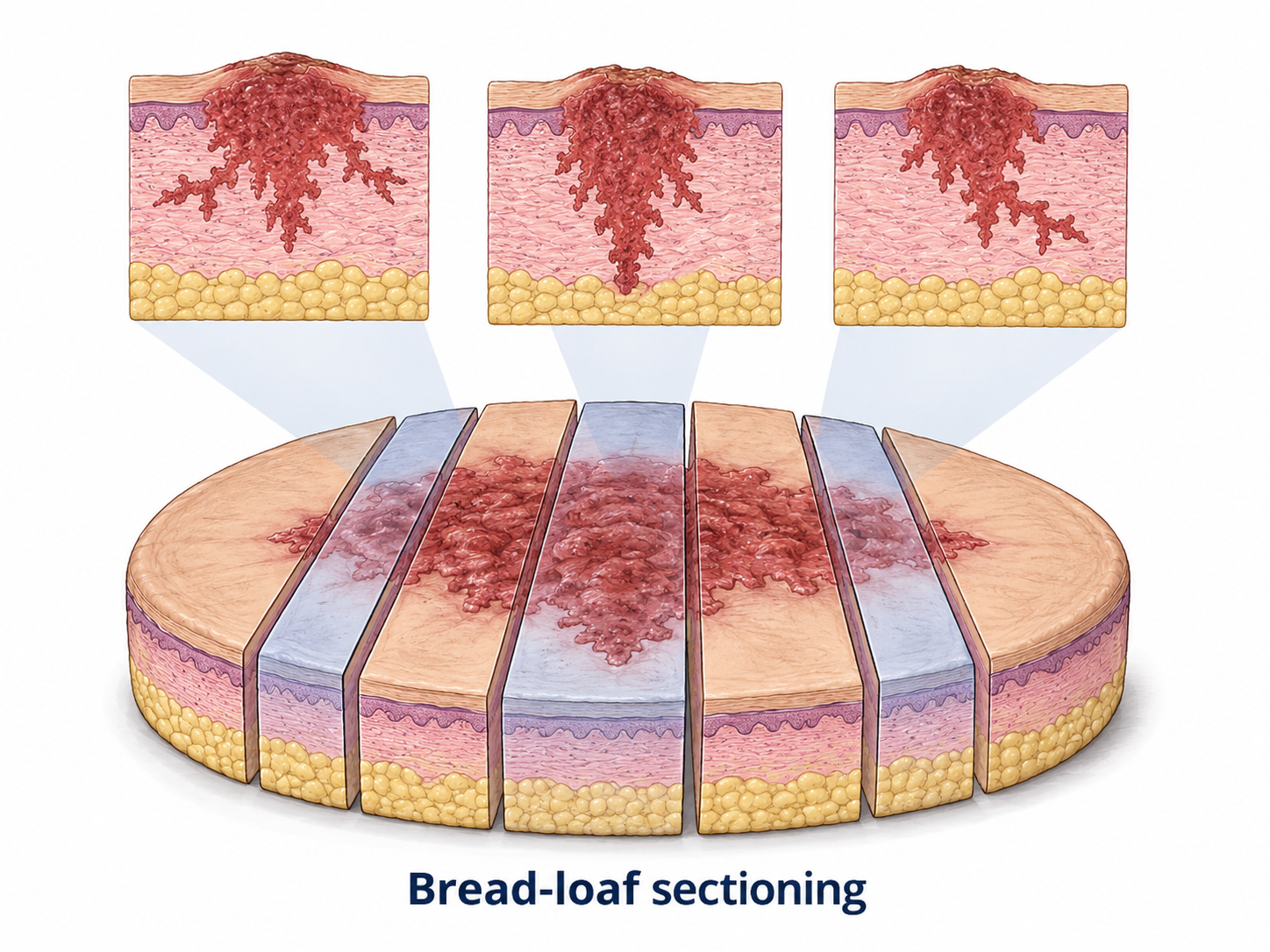
Standard excision
Representative vertical sections
Mohs / PDEMA
Peripheral + deep en face assessment
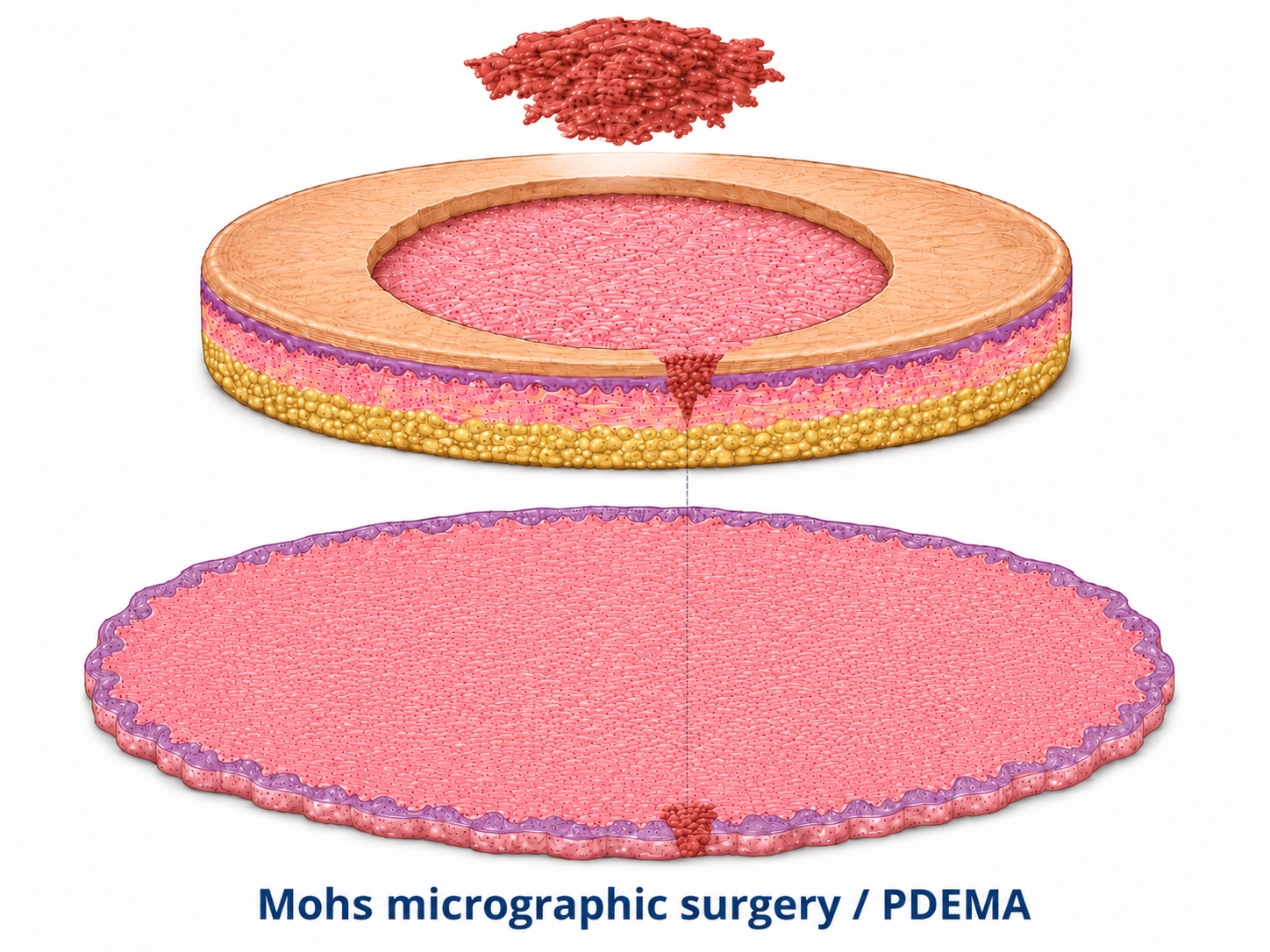
Key distinction: standard excision=margin sampling; PDEMA =complete assessment.
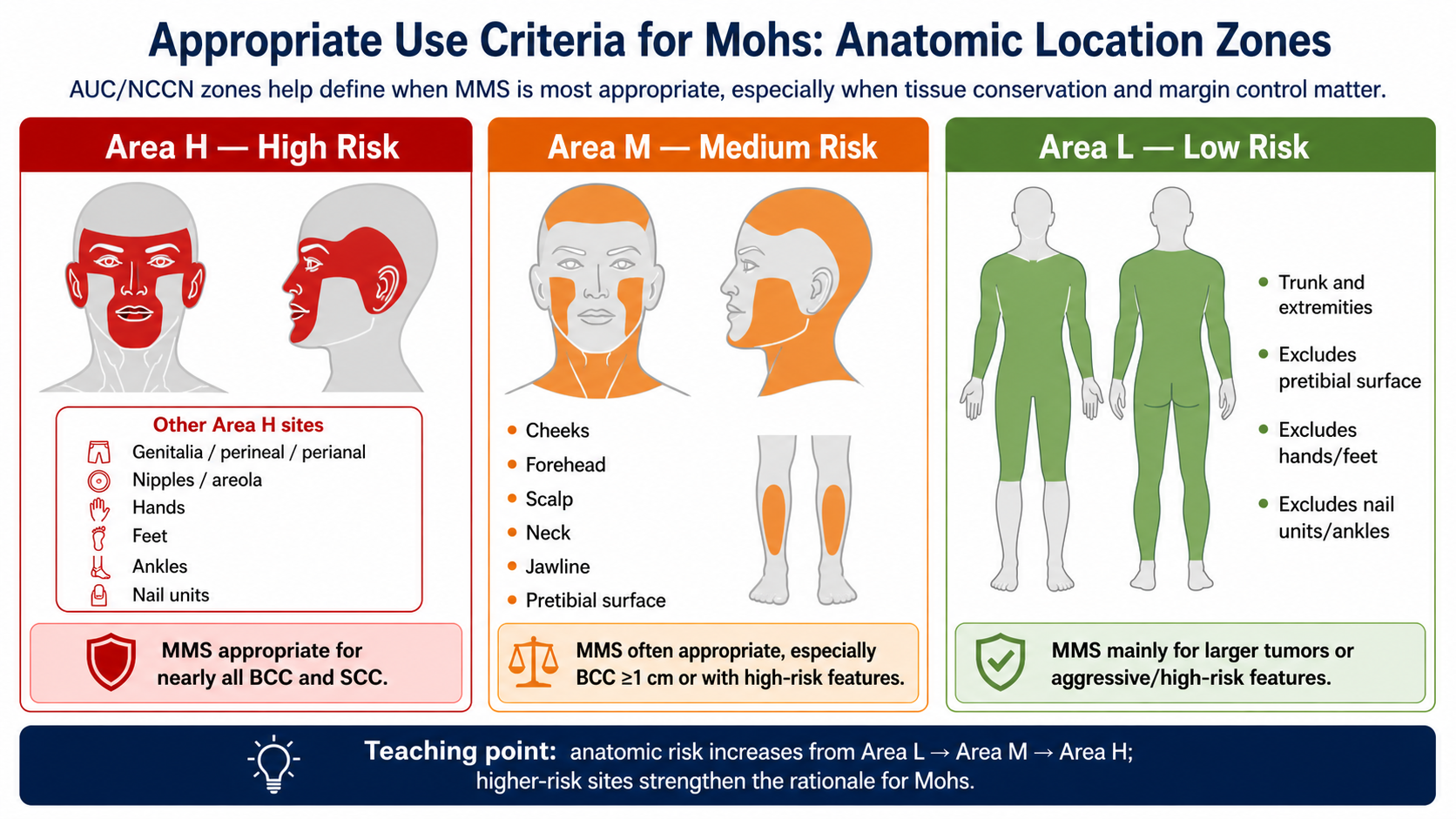
Why Location Matters
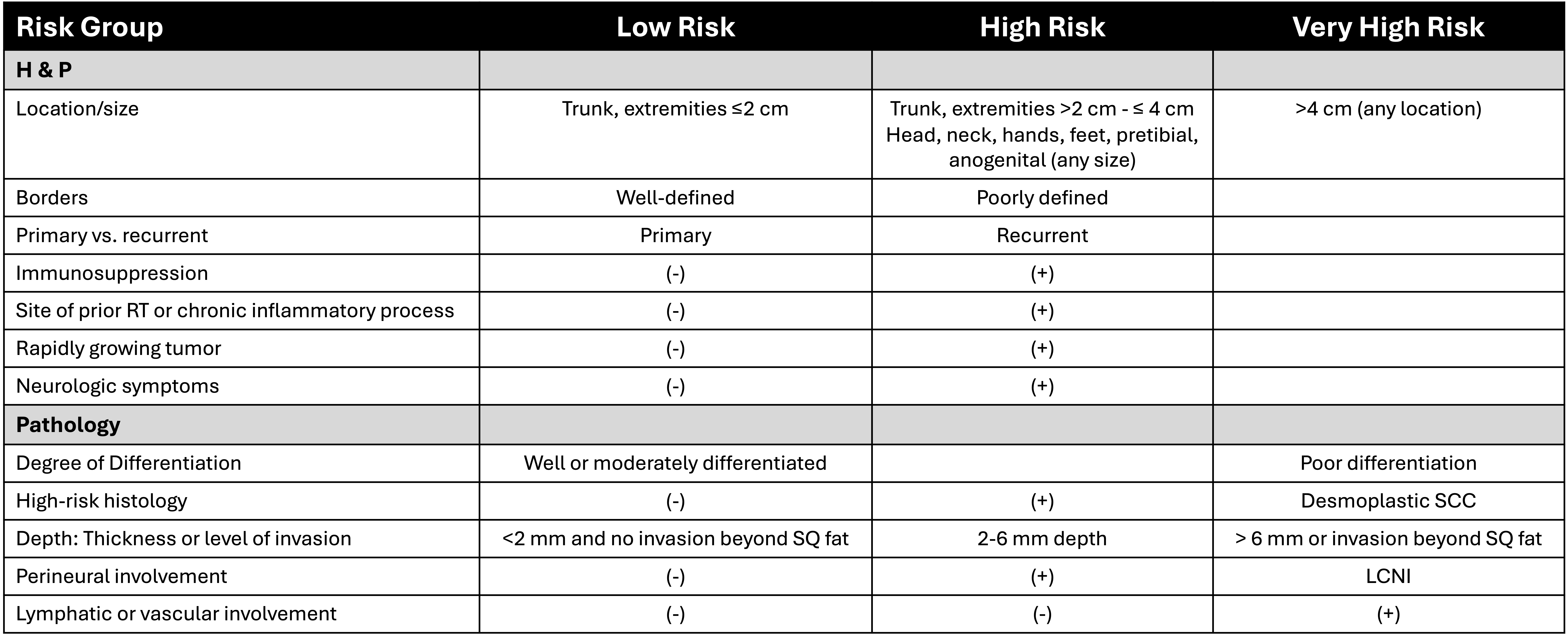
NCCN Risk Stratification
Case 5: Large Forehead CSCC
An 82-year-old woman with numerous prior NMSCs presents with a rapidly growing lesion on the left forehead.
Physical exam:
- 4.1 cm
- No clinical adenopathy
Biopsy shows:
- Poorly-differentiated CSCC

Question: cut & close, or consult?